{kind=link}
{kind=link}
Last updated: 22-03-2024 for Round 18 Scenarios.
https://covid19scenariomodelinghub.org/viz.html
Round 17: Scenario Descriptions and Model Details
Even the best models of emerging infections struggle to give accurate forecasts at time scales greater than 3-4 weeks due to unpredictable drivers such as a changing policy environment, behavior change, the development of new control measures, and stochastic events. However, policy decisions around the course of emerging infections often require projections in the time frame of months. The goal of long-term projections is to compare outbreak trajectories under different scenarios, as opposed to offering a specific, unconditional estimate of what "will" happen. As such, long-term projections can guide longer-term decision-making while short-term forecasts are more useful for situational awareness and guiding immediate response. The need for long-term epidemic projections is particularly acute in a severe pandemic, such as COVID-19, that has a large impact on the economy; for instance, economic and budget projections require estimates of outbreak trajectories in the 3-6 month time scale.
From weather to infectious diseases, it has been shown that synergizing results from multiple models gives more reliable projections than any one model alone. In the COVID-19 pandemic this approach has been exemplified by the COVID-19 Forecast Hub, which combines the results of over 30 models (see a report on the first wave of the pandemic). Further, a comparison of the impact of interventions across 17 models has illustrated how any individual model can grossly underestimate uncertainty, while ensemble projections can offer robust projections of COVID-19 the course of the epidemic under different scenarios at a 6-month time scale.
The COVID-19 Forecasting Hub provides useful and accurate short-term forecasts, but there remains a lack of publicly available model projections at 3-6 month time scale. Some single models are available online (e.g., IHME, or Imperial College), but a decade of infectious disease forecasts has demonstrated that projections from a single model are particularly risky. Single model projections are particularly problematic for emerging infections where there is much uncertainty about basic epidemiological parameters (such as the waning of immunity), the transmission process, future policies, the impact of interventions, and how the population may react to the outbreak and associated interventions. There is a need for generating long-term COVID-19 projections combining insights from different models and making them available to decision-makers, public health experts, and the general public. We plan to fill this gap by building a public COVID-19 Scenario Hub to harmonize scenario projections in the United States.
We have specified a set of scenarios and target outcomes to allow alignment of model projections for collective insights. Scenarios have been designed in consultation with academic modeling teams and government agencies (e.g., CDC).
The COVID-19 Scenario Modeling Hub is be open to any team willing to provide projections at the right temporal and spatial scales, with minimal gatekeeping. We only require that participating teams share point estimates and uncertainty bounds, along with a short model description and answers to a list of key questions about design. A major output of the projection hub would be ensemble estimates of epidemic outcomes (e.g., cases, hospitalization and/or deaths), for different time points, intervention scenarios, and US jurisdictions.
Those interested to participate, please read the README file and email us at [email protected].
Model projections should be submitted via pull request to the data-processed folder of this GitHub repository. Technical instructions for submission and required file formats can be found here.
Round 18 focuses on the impact of different COVID-19 vaccination strategies with reformulated boosters combined with differing levels of antigenic drift. This round will follow closely the layout of Round 17, but with more consideration of population groups at high-risk for severe disease (of any age). The timeframe of projection will be Sun April 28, 2024 to Sat April 26, 2025 (52 weeks).
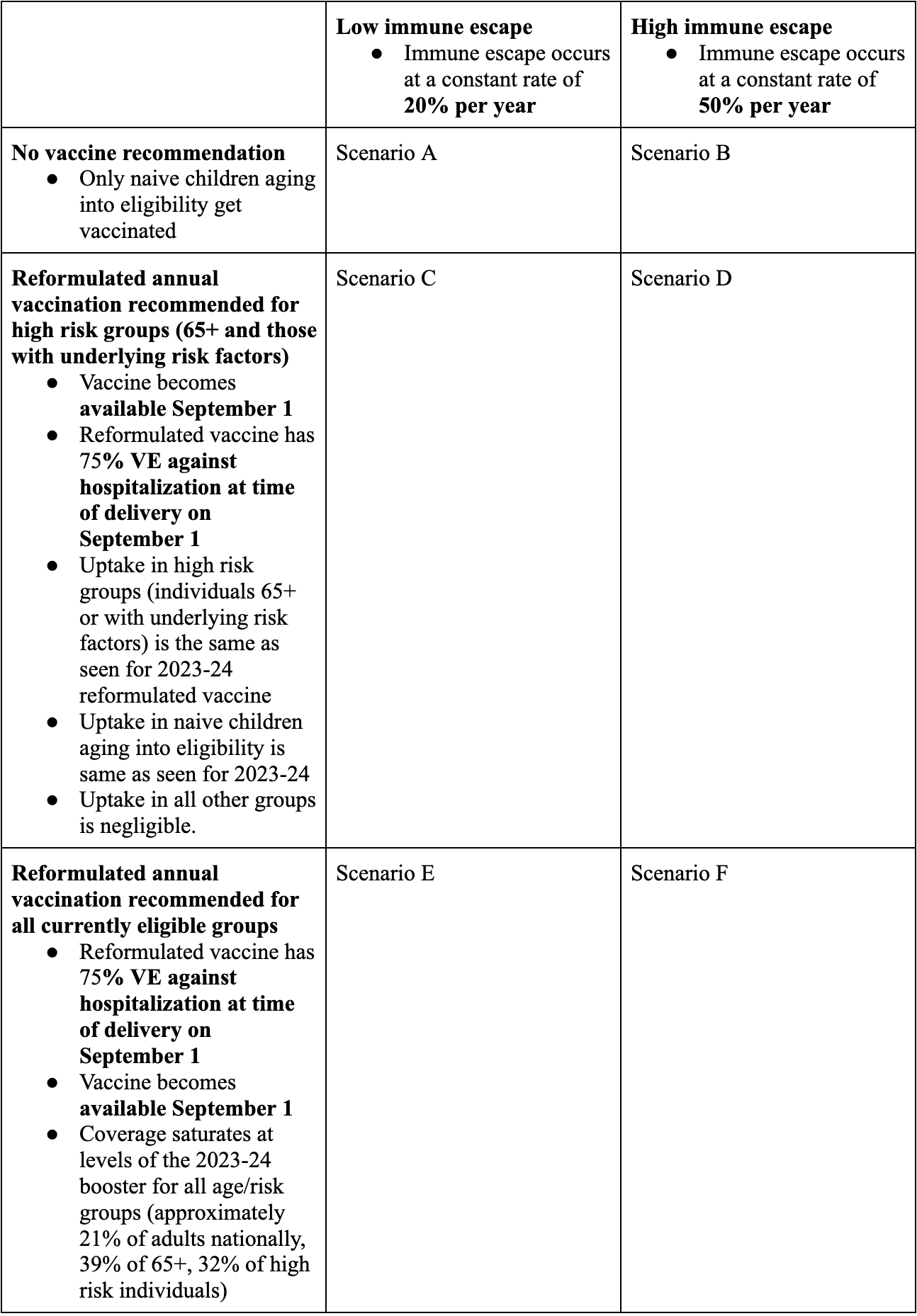
In all scenarios, boosters are reformulated to match the predominant variants circulating on June 15, 2024. Teams should use VE against COVID19 hospitalization = 75% at time of release on Sep 1, 2024, in line with a recent study from Denmark. This VE is equivalent to a vaccine trial that would be performed on September 1 in populations with varying levels of prior immunity at trial enrollment. Hence, vaccinated individuals would have a 75% reduced risk of hospitalization compared to unvaccinated individuals on average in this trial, if VE was estimated a few days after Sepetember 1st. Importantly, this stated hospitalization reduction includes the combined effects of protection against infection and protection against hospitalization given (breakthrough) infection. We note that this is a departure from earlier COVID-19 rounds where we stipulated VE against symptomatic disease. Based on available evidence, we suggest that teams choose VE against infection in the range 35-57% at time of release on Sept 1, 2024 (see Google Docs for detailed studies).
As in Round 17, immune escape may decrease the effective VE against
hospitalization, starting on September 1. While immune escape against
infection should be modeled as stipulated in the scenarios (20/50% a year),
immune escape against severe disease is at teams’ discretion.
Further, waning of (vaccine-induced and natural) immunity against infection is
required, with parameters at teams discretion (3-10mo waning time, 40-60%
reduction against baseline protection levels in waned state). Waning of
vaccine-induced immunity against severe disease remains at teams discretion
(but if present should wane at slower timescale than against infection).
No recommendation (scenarios A & B): There is no future recommendation to get additional booster doses or receive additional vaccination. Teams should not model any future vaccination except among those not previously vaccinated, specifically children aging into eligibility (i.e, at 6 months of age). Without recommendation, vaccines will not be covered by insurance or other sources.
Annual vaccination with reformulated booster recommended for high risk groups (65+ and those with underlying risk factors) (scenarios C & D): Uptake of annual reformulated booster in high-risk groups (65+ and other individuals with underlying risk factors for severe COVID-19 outcomes) follows uptake observed for the booster dose during the 2023-24 season. Vaccination among others outside of high risk groups should be negligible, except among infants aging into eligibility (at 6 months). For non-recommended groups, it should be assumed without recommendation these will not be covered by insurance or other health care funding and thus will not be received. Uptake data from the 2023-24 season in 65+ and high-risk groups will be provided.
Annual vaccination with reformulated booster recommended for currently eligible groups (ages 6 months and older)(scenarios E & F): Uptake of annual reformulated booster in all groups follows uptake observed for the booster dose during the 2023-24 season. Uptake data from the 2023-24 season will be provided.
In this round, we assume that high-risk populations, of any age, are included in booster recommendations in scenarios C, D, E, & F. We define high-risk groups as those with underlying conditions putting them at increased risk of severe outcomes from COVID-19. Data on the population size and vaccine coverage of high and low risk groups is provided by state and age in GitHub. Teams can choose to adjust VE for high-risk and low-risk groups based on available evidence, although the population-level average VE against hospitalization should equal 75% on September 1. Data on increased risk of COVID-19 hospitalization from high risk groups can be found here.
Projected vaccine coverage curves for 2024-25 season, by age, state, and high-risk group, with population sizes of relevant age groups, are available in the round_resources/round18 folder.
The SARS-CoV-2 virus is presumed to evolve away from existing immunity at a roughly constant rate of 20% or 50% per year, depending on the scenario. For example, in the 20% immune escape scenario, a vaccine formulated for a variant circulating on June 15th would have a VE of 0.9 times the VE at reformulation when administered six months later on December 15th.
Similarly, immune escape will affect protection conferred by natural infection. Let’s assume an individual is infected on June 15, 2024 and this infection confers X% protection against symptoms, compared to an individual who has not been recently infected. If this individual was instantaneously transported a year later, on June 15, 2025, with their antibodies from the 2024 infection intact, this individual's protection against variants circulating on June 15, 2025 would be X * 0.8 in the 20% immune escape scenario. In this thought experiment, the decay of protection would solely be due to the effects of immune escape. In reality, moving away from the thought experiment, if this individual actually lived throughout an entire year without a new infection between June 2024 and June 2025, then their effective immunity on June 15, 2025 will be the combined effects of antibody waning (at a rate and plateau left at teams’ discretion) and immune escape (prescribed by each scenario).
Teams should note that the impact of immune escape is separate from the impact of waning immunity (especially because the impact of immune escape affects infection and vaccination differently), although these processes may be implemented similarly in models.
It is left to the teams’ discretion how to implement immune escape in their models. Teams may choose to introduce new discrete variants with levels of immune escape consistent with the scenario definition, so long as these occur frequently, or may implement gradual escape of existing variants.
Teams must incorporate waning of immunity against infection. The median waning time of protection against infection should range between 3-10 months (this should not be read to mean that waning is to complete loss of protection, see below). Teams can sample this range, or use any value within this range as a point estimate. Teams can consider differences in waning of natural and vaccine-induced immunity, or in waning after Omicron infection vs waning from other types of SARS-CoV-2 exposures; however the median waning time should remain within the 3-10 month range.
The rate and levels of waning are left to the best scientific discretion of the teams. We recommend that in the waned classes, teams consider a reduction from baseline levels of protection ranging between 40% and 60%, corresponding to x0.60 and x0.40 of the baseline levels reported immediately after exposure (vaccination or infection).
Teams may incorporate waning of immunity against severe disease, however the timescale of waning against severe disease must be slower than the timescale of waning against infection.
It is important that all scenario simulations share the same values (or ranges of values) for the proportion of population in different immune classes at the start of projections. Similarly, waning immunity assumptions should be shared across scenarios (including timescale of immunity decline and plateau reached after immunity has waned, if any). To do so, teams should ensure that the calibration step uses similar immune escape and waning immunity parameters. Only by using assumptions that lead to starting conditions for population immunity that effectively come from a shared distribution across scenarios and by having the same waning immunity assumptions (or shared distribution of waning immunities) apply to all scenarios, can we evaluate the impact of different immune escape and vaccine assumptions in the projection period. If past immune escape and/or waning immunity parameters are unobservable from the recent data, estimates can be drawn from the literature to help with calibration. It is also acceptable to use the midpoint of the immune escape scenario assumptions (35%, midpoint between 20% and 50%) for calibration of immune escape in the recent past.
Teams should assume no new variants are introduced, other than those implied by the levels of immune escape specified in the scenarios. Treatment of variants existing at the start of the projection period is left to the discretion of the teams. Intrinsic transmissibility and severity of disease in a naive individual is assumed to be constant across all currently-circulating and future variants.
Teams should include their best estimate of COVID-19 seasonality in their model, but we do not prescribe a specific level of seasonal forcing. Teams should consider the observed resurgence of COVID-19 in the fall of 2023, particularly in Southern states, and in winter 2023-24 throughout the country. If feasible, we ask that teams check that their models are able to reproduce the observed timing of COVID-19 activity in the past year in their calibration step.
Teams should NOT include reactive changes in NPIs imposed by health authorities to curb transmission, e.g., reinstatement of mask mandates, or closure of schools and businesses. However, teams can incorporate inherent changes in population behavior in response to increasing or decreasing incidences (eg, changes in contacts or masking), if these changes were inferred from earlier phases of the pandemic and are already part of the model.
Database tracking of NPIs: teams may use their own data if desired, otherwise we recommend the following sources as a common starting point:
- Coronavirus Government Response Tracker | Blavatnik School of Government (ox.ac.uk)
- Coronavirus State Actions - National Governors Association (nga.org)
The mix of circulating strains at the start of the projection period is at the discretion of the teams based on their interpretation/analysis of the available data. Variation in initial prevalence between states is left at teams’ discretion.
Targets will be similar to Round 17 and consist of weekly state- and national-level COVID-19 hospitalizations and deaths. We no longer request case projections. Ascertainment of hospitalizations and deaths will proceed at the same level as they were at the start of the projection period. HHS protect will be used as the source of hospitalization data (note that HHSprotect will temporarily go offline at the end of April 2024). NCHS will be used as the source of gold-standard death data. Note that NCHS data source counts deaths on the dates they occurred, not on the date they were reported. In accordance with the data, the death target should give deaths on the date they occur.
Both weekly state- and national-level COVID-19 hospitalizations and deaths should be provided for the following age groups: 0-64, 65+ and overall population
Whether or not to include demographic dynamics (aging, birth) is at the discretion of the teams.
All of the teams' specific assumptions should be documented in meta-data and abstract.
Projection Time Horizon: We consider a one-year projection period.
| Scenario | Scenario name | Scenario ID for submission file ('scenario_id') |
|---|---|---|
| Scenario A. No booster, low immune escape | noBoo_lowIE | A-2024-03-01 |
| Scenario B. No booster, high immune escape | noBoo_highIE | B-2024-03-01 |
| Scenario C. 65+ booster, low immune escape | 65Boo_lowIE | C-2024-03-01 |
| Scenario D. 65+ booster, high immune escape | 65Boo_highIE | D-2024-03-01 |
| Scenario E. All booster, low immune escape | allBoo_lowIE | E-2024-03-01 |
| Scenario F. All booster, high immune escape | allBoo_highIE | F-2024-03-01 |
-
Due date: Tue Apr 30, 2024
-
End date for fitting data: April 27, 2024 (no later than April 27, no earlier than April 14)
-
Start date for scenarios: April 28, 2024 (first date of simulated transmission/outcomes)
-
Simulation end date: April 26, 2025 (52-week horizon)
Submission Target
- Weekly Incident Deaths
- Weekly Incident Hospitalization
Other submission requirements
-
Geographic scope: state-level and national projections
-
Results:
- Simulation trajectories: We ask that teams submit a sample of 100 to 300 simulation replicates. Simulations should be sampled in such a way that they will be most likely to produce the uncertainty of the simulated process. For some models, this may mean a random sample of simulations, for others with larger numbers of simulations, it may require weighted sampling. Trajectories will need to be paired across horizon and age groups (eg, for a given model, location, scenario and week, all age data for simulation 1 corresponds to the sum of age-specific estimates for simulation 1).
- Projection quantiles for incident outcomes are optional but encouraged.
Similarly projections of cumulative outcomes (either as quantiles or cumulative
trajectories) are optional.
- Weekly incident deaths
- Weekly incident hospitalizations
- Weekly cumulative deaths since simulation start (No longer cumulative since the start of the pandemic due to the lag in FluView baseline data)
- Weekly cumulative hospitalizations since simulation start
- For teams who wish to submit quantiles, the format is in accordance with prior rounds. We ask for the following quantiles: 0.01, 0.025, 0.05, every 5% to 0.95, 0.975, and 0.99. Mean is optional.
- Weeks will follow epi-weeks (Sun-Sat) dated by the last day of the week
- Submission file type: gz.parquet (from Apache Arrow) is now required. The submission file can be partitioned by "origin_date" and "target". For more information, please consult the associated README
-
Abstract: We require a brief abstract describing model assumptions and results, from all teams.
-
Metadata: We require a brief metadata form, from all teams.
- Round 2 Scenarios
- Round 3 Scenarios
- Round 4 Scenarios
- Round 5 Scenarios
- Round 6 Scenarios
- Round 7 Scenarios
- Round 8 Scenarios
- Round 9 Scenarios
- Round 10 Scenarios
- Round 11 Scenarios
- Round 12 Scenarios
- Round 13 Scenarios
- Round 14 Scenarios
- Round 15 Scenarios
- Round 16 Scenarios
- Round 17 Scenarios
Groups interested in participating can submit model projections for each scenario in a PARQUET file formatted according to our specifications, and a metadata file with a description of model information. See here for technical submission requirements.
Until round 17, we used the daily reports containing COVID-19 cases and deaths data from the JHU CSSE group as the gold standard reference data for cases and deaths in the US. We will use the distribution of the JHU data as provided by the COVIDcast Epidata API maintained by the Delphi Research Group at Carnegie Mellon University.
For COVID-19 hospitalizations, we used the HealthData.gov COVID-19 Reported Patient Impact and Hospital Capacity by State Timeseries. These data are released weekly although, sometimes, are updated more frequently. A supplemental data source with daily counts that should be updated more frequently (typically daily) but does not include the full time-series is HealthData.gov COVID-19 Reported Patient Impact and Hospital Capacity by State.
Starting Round 13 (W12-2022), for COVID-19 hospitalizations, we will use the same truth data as the COVID-19 Forecast Hub, i.e., the hospitalization data from the HHS for example the HealthData.gov COVID-19 Reported Patient Impact and Hospital Capacity by State Timeseries and HealthData.gov COVID-19 Reported Patient Impact and Hospital Capacity by State. We will use the distribution of the HHS data as provided by the COVIDcast Epidata API maintained by the Delphi Research Group at Carnegie Mellon University.
Starting round 17 (March 2023), we use National Center for Health Statistics (NCHS) Mortality Surveillance Data data for weekly incidence COVID-19 deaths extracted from the FluView Interactive - Mortality CDC dashboard. These data are weekly and pertain to date of death, not report date. Due to the delay and backfilling of these data, the cumulative death target will also now start from the date of projection (instead of cumulative since pandemic start).
We aim to combine model projections into an ensemble.
We are grateful to the teams who have generated these scenarios. The groups have made their public data available under different terms and licenses. You will find the licenses (when provided) within the model-specific folders in the data-processed directory. Please consult these licenses before using these data to ensure that you follow the terms under which these data were released.
All source code that is specific to the overall project is available under an open-source MIT license. We note that this license does NOT cover model code from the various teams or model scenario data (available under specified licenses as described above).
Those teams interested in accessing additional computational power should contact Katriona Shea at [email protected]{.email}.
Teams are encouraged to share code they think will be useful to other teams via the github repo. This directory can be found in code_resources. It currently contains code to: - Pull age-specific, state-specific, time-series data on vaccination in the US from the CDC API. get_cdc_stateagevacc.R
- Johns Hopkins ID Dynamics COVID-19 Working Group --- COVID
Scenario
Pipeline
- Joseph C. Lemaitre (UNC), Joshua Kaminsky (Johns Hopkins Infectious Disease Dynamics), Claire P. Smith (Johns Hopkins Infectious Disease Dynamics), Sara Loo (Johns Hopkins Infectious Disease Dynamics), Clif McKee (Johns Hopkins Infectious Disease Dynamics), Alison Hill (Johns Hopkins Infectious Disease Dynamics), Sung-mok Jung (UNC), Erica Carcelen (Johns Hopkins Infectious Disease Dynamics), Koji Sato (Johns Hopkins Infectious Disease Dynamics), Elizabeth C. Lee (Johns Hopkins Infectious Disease Dynamics), Justin Lessler (UNC), Shaun Truelove (Johns Hopkins Infectious Disease Dynamics)
- Johns Hopkins University Applied Physics Lab ---
Bucky
- Matt Kinsey (JHU/APL), Kate Tallaksen (JHU/APL), R.F. Obrecht (JHU/APL), Laura Asher (JHU/APL), Cash Costello (JHU/APL), Michael Kelbaugh (JHU/APL), Shelby Wilson (JHU/APL), Lauren Shin (JHU/APL), Molly Gallagher (JHU/APL), Luke Mullany (JHU/APL), Kaitlin Lovett (JHU/APL)
- Karlen Working Group ---
pypm
- Dean Karlen (University of Victoria and TRIUMF)
- Northeastern University MOBS Lab --- GLEAM
COVID
- Matteo Chinazzi (Laboratory for the Modeling of Biological and Socio-technical Systems, Northeastern University, Boston, MA), Jessica T. Davis (Laboratory for the Modeling of Biological and Socio-technical Systems, Northeastern University, Boston, MA), Kunpeng Mu (Laboratory for the Modeling of Biological and Socio-technical Systems, Northeastern University, Boston, MA), Xinyue Xiong (Laboratory for the Modeling of Biological and Socio-technical Systems, Northeastern University, Boston, MA), Ana Pastore y Piontti (Laboratory for the Modeling of Biological and Socio-technical Systems, Northeastern University, Boston, MA), Alessandro Vespignani (Laboratory for the Modeling of Biological and Socio-technical Systems, Northeastern University, Boston, MA)
- University of Southern California --- SI
kJalpha
- Ajitesh Srivastava, Majd Al Aawar
- University of Virginia ---
adaptive
- Przemyslaw Porebski (UVA), Srini Venkatramanan (UVA), Bryan Lewis (UVA), Aniruddha Adiga (UVA), Brian Klahn (UVA), Benjamin Hurt (UVA), Jiangzhuo Chen (UVA), Anil Vullikanti (UVA), Madhav Marathe (UVA)
- Oliver Wyman's Pandemic
Navigator
- Ugur Koyluoglu, Dan Siegel
- Columbia University - Age-Stratified
Model
- Marta Galanti (CU), Teresa Yamana (CU), Sen Pei (CU), Jeffrey Shaman (CU)
- University of North Carolina at Charlotte -
hierbin
- Shi Chen (UNC Charlotte Department of Public Health Sciences & School of Data Science), Rajib Paul (UNC Charlotte Department of Public Health Sciences and School of Data Science), Daniel Janies (UNC Charlotte Department of Bioinformatics and Genomics), Jean-Claude Thill (UNC Charlotte Department of Geography and Earth Sciences and School of Data Science)
- Institute for Health Metrics and Evaluation -- IHME COVID model
deaths
unscaled
- Robert C Reiner, Joanne Amlag, Ryan M. Barber, James K. Collins, Peng Zheng, James Albright, Catherine M. Antony, Aleksandr Y. Aravkin, Steven D. Bachmeier, Marlena S. Bannick, Sabina Bloom, Austin Carter, Emma Castro, Kate Causey, Suman Chakrabarti, Fiona J. Charlson, Rebecca M. Cogen, Emily Combs, Xiaochen Dai, William James Dangel, Lucas Earl, Samuel B. Ewald, Maha Ezalarab, Alize J. Ferrari, Abraham Flaxman, Joseph Jon Frostad, Nancy Fullman, Emmanuela Gakidou, John Gallagher, Scott D. Glenn, Erik A. Goosmann, Jiawei He, Nathaniel J. Henry, Erin N. Hulland, Benjamin Hurst, Casey Johanns, Parkes J. Kendrick, Samantha Leigh Larson, Alice Lazzar-Atwood, Kate E. LeGrand, Haley Lescinsky, Emily Linebarger, Rafael Lozano, Rui Ma, Johan Månsson, Ana M. Mantilla Herrera, Laurie B. Marczak, Molly K. Miller-Petrie, Ali H. Mokdad, Julia Deryn Morgan, Paulami Naik, Christopher M. Odell, James K. O'Halloran, Aaron E. Osgood-Zimmerman, Samuel M. Ostroff, Maja Pasovic, Louise Penberthy, Geoffrey Phipps, David M. Pigott, Ian Pollock, Rebecca E. Ramshaw, Sofia Boston Redford, Sam Rolfe, Damian Francesco Santomauro, John R. Shackleton, David H. Shaw, Brittney S. Sheena, Aleksei Sholokhov, Reed J. D. Sorensen, Gianna Sparks, Emma Elizabeth Spurlock, Michelle L. Subart, Ruri Syailendrawati, Anna E. Torre, Christopher E. Troeger, Theo Vos, Alexandrea Watson, Stefanie Watson, Kirsten E. Wiens, Lauren Woyczynski, Liming Xu, Jize Zhang, Simon I. Hay, Stephen S. Lim & Christopher J. L. Murray
- University of Virginia -
EpiHiper
- Jiangzhuo Chen (UVA), Stefan Hoops (UVA), Parantapa Bhattacharya (UVA), Dustin Machi (UVA), Bryan Lewis (UVA), Madhav Marathe (UVA)
- University of Notre Dame -
FRED
- Guido Espana, Sean Cavany, Sean Moore, Alex Perkins
- University of Florida -
ABM
- Thomas Hladish (University of Florida), Alexander Pillai (University of Florida), Kok Ben Toh (Northwestern University), Ira Longini Jr. (University of Florida)
- North Carolina State University -
COVSIM
- Erik Rosenstrom (North Carolina State University), Sebastian Rodriguez Cartes (North Carolina State University), Julie Swann (North Carolina State University), Julie Ivy (North Carolina State University), Maria Mayorga (North Carolina State University)
- University of Texas at Austin -
ImmunoSEIRS
- Kaiming Bi (Lead modeler, University of Texas at Austin), Anass Bouchnita (University of Texas at El Paso), Shraddha R Bandekar (University of Texas at Austin), Spencer Fox (University of Georgia), Lauren Ancel Meyers (Senior author, University of Texas at Austin), and the UT COVID-19 Modeling Consortium
- Justin Lessler, University of North Carolina
- Katriona Shea, Penn State University
- Cécile Viboud, NIH Fogarty
- Shaun Truelove, Johns Hopkins University
- Claire Smith, Johns Hopkins University
- Emily Howerton, Penn State University
- Nick Reich, University of Massachussetts at Amherst
- Harry Hochheiser, University of Pittsburgh
- Michael Runge, USGS
- Lucie Contamin, University of Pittsburgh
- John Levander, University of Pittsburgh
- Jessi Espino, University of Pittsburgh
- Sara Loo, Johns Hopkins University
- Erica Carcelen, John Hopkins University
- Sung-mok Jung, University of North Carolina
- Samantha Bents, NIH Fogarty
- Katie Yan, Penn State University
- Wilbert Van Panhuis, University of Pittsburgh
- Jessica Kerr, University of Pittsburgh
- Luke Mullany, Johns Hopkins University
- Kaitlin Lovett, John Hopkins University
- Michelle Qin, Harvard University
- Tiffany Bogich, Penn State University
- Rebecca Borchering, Penn State University